 |
MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS |
| << DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:Amnesia |
| MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS >> |
Abnormal
Psychology PSY404
VU
Lesson
42
MENTAL
RETARDATION AND DEVELOPMENTAL
DISORDERS
Mental
Retardation
Example:
A is a teenage boy who has
shown problems in intellectual and
social functioning; he
needs
help
to eat, to bath and to dress
up.
·
What
is mental retardation?
·
Why
study mental
retardation?
·
All
people with mental retardation have
impaired intellectual abilities, but they vary widely
in
academic
ability, social functioning,
and life skills.
·
Some
people with profound retardation require
total care and live
their entire lives in
institutions.
·
However,
most people with mental retardation
learn self-care and vocational
skills that allow
them
to
live in the community.
·
Many
people with mental retardation suffer
from emotional difficulties, a
fact that is overlooked
all
too
often.
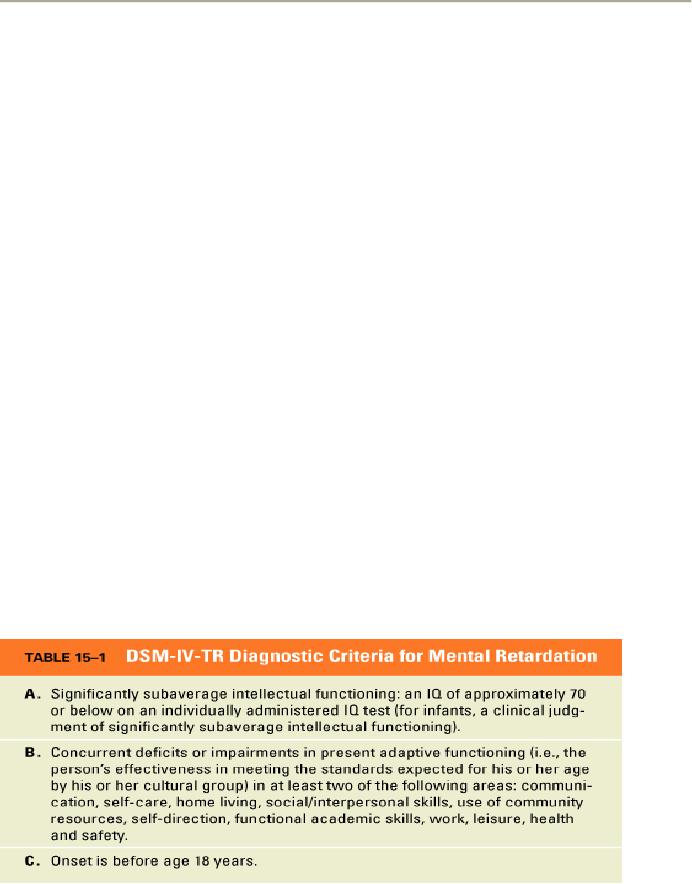
What
is Mental Retardation?
Mental
retardation is
1-
Significant limitations in intellectual
functioning
2-
Significant limitations in adaptive
functioning
3-
Onset before age 18
years.
·
The
American Association on Mental Retardation (AAMR), the
leading organization for
professionals
concerned with mental retardation,
defines mental retardation somewhat
differently
than
DSM-IV-TR. However, both
definitions generally agree on the
three major criteria for
mental
retardation,
mentioned above.
·
The
AAMR and DSM-IV-TR both
define subaverage intellectual
functioning in terms of a score
on
an
individualized intelligence
test, a
standardized measure for
assessing intellectual ability.
·
Intelligence
tests yield a score called
the intelligence quotient, or IQ, the
test's rating of an
individual's
intellectual ability.
Symptoms
of Mental Retardation
Defining
intelligence
can be
controversial, and definitions and
measures of intellectual ability
have
changed
over the years. Early
versions of intelligence tests derived an IQ by
dividing the individual's
"mental
age" by his or her chronological
age. Mental age was
determined by comparing an
individual's
test
results with the average obtained
for various age groups.
Contemporary intelligence tests
have
208
Abnormal
Psychology PSY404
VU
abandoned
the concept of mental age
and instead have adopted the
concept of the "deviation
IQ".
According
to this theory of "deviation IQ",
intellectual ability follows the normal
distribution in the
population,
a bell-shaped frequency
distribution.
The
individual's IQ is determined based on
how the person scores on an intelligence
test relative to the
norms
for his or her age group. IQ
tests are widely used, and
they have demonstrated value
for
predicting
performance in school. Moreover, IQ is a
trait that is stable over
time.
Despite
the value of IQ tests in predicting
academic performance, a number of
important questions
have
been raised about them. One
of the most controversial questions is whether
intelligence tests are
"culture-fair."
Culture-fair tests contain material
that is equally familiar to people
who differ in their
ethnicity,
native language, or immigrant status.
Tests that are culturally
biased contain
language, examples,
or
other assumptions that favor
one ethnic group, particularly members of the
majority group, over
another.
Another
controversy is how well intelligence is
measured among people with
mental retardation. Many
people
with mental retardation have
sensory or physical disabilities that
impede their performance
on
standard
IQ tests; thus they must
take tests that are
not influenced by their particular
disability. Despite
the
difficulties, evidence indicates that, if
anything, the IQ test scores of people
with mental retardation
are
more
reliable
and valid than IQ scores in
the normal range. Common sense,
social sensitivity, and
"street
smarts" are also part of
what most of us would consider
intelligence, and they are not
measured
by
IQ tests.
Both
the AAMR and DSM recognize
that intelligence is more than an IQ
score; thus they include
adaptive
behavior as a part of their
definitions of mental retardation. The
most basic concern
about
intelligence
tests is the most important
one: What is intelligence?
Intelligence tests measure
precisely
what
their original developer, Alfred
Binet, intended them to
measure: potential for
school
achievement.
IQ tests predict school achievement
fairly well. However, school
achievement is not
the
same
as "intelligence."
The
AAMR suggests that adaptive
behavior includes conceptual,
social, and practical
skills.
·
Conceptual
skills focus
largely on community self-sufficiency,
and incorporate communication,
functional
academics, self-direction, and health and
safety from
DSM-IV-TR.
·
Social
skills focus
on understanding how to conduct oneself in
social situations and include
social
skills
and leisure from the
DSM-IV-TR list.
·
Practical
skills focus
on the tasks of daily living
and include self-care, home
living, community use,
health
and safety, and work
from the DSM-IV-TR.
Adaptive
skills are difficult to
quantify. As with the definition of
IQ, the AAMR now defines
a
significant
limitation in adaptive behavior as a
score that is two standard
deviations below the mean on
a
standardized measure of adaptive
behavior in conceptual, social, or
practical skills.
An
argument has been made
for defining retardation solely on the
basis of intelligence testing,
because
current
measures of adaptive skills
are imprecise. However, the adaptive
skills criterion highlights
the
importance
of assessing life functioning in
borderline cases, as well as the
need for services
among
people
with mental retardation.
The
third criterion for defining
mental retardation is onset before 18
years of age. This
criterion
excludes
people whose deficits in intellect and
adaptive skills begin later in life as a
result of brain
injury
or
disease. People with mental
retardation have not lost skills they
once had mastered, nor
have they
experienced
a notable change in their
condition.
209
Abnormal
Psychology PSY404
VU
Diagnosis
of Mental Retardation
·
In
1866, the British physician
Langdon Down first described
a subgroup of children with
mental
retardation
who had a characteristic
appearance.
·
Down's
classification helped subsequent
scientists to establish a specific
etiology for what we
now
know
as Down syndrome.
·
The
creation of IQ tests in the early
twentieth century also greatly
furthered the classification of
mental
retardation.
·
Once
academic potential could be
measured, controversy grew about what IQ
score cutoff should
define
mental retardation.
·
The
AAMR has set the cutoff at
two standard deviations below the mean
(70).
·
Today,
mental retardation can be classified
according to two different
criteria.
·
One
criterion is based on IQ scores; the
other is according to known or
presumed etiology.
·
The
AAMR uses a multiaxial
diagnosis of mental retardation in which
health, including etiological
factors,
is rated on a separate
axis.
·
A
more controversial aspect of the AAMR
sub-classification is the ratings of four
levels of
"intensity
of needed support" across
nine different areas of
functioning.
·
Today,
mental retardation can be classified
according to two different
criteria.
·
One
criterion is based on IQ scores; the
other is according to known or
presumed etiology.
The
goal in rating support intensities is to
acknowledge the diversity of skills and
needs among people
with
mental
retardation both as people and for
treatment planning.
In
adopting the support intensities
approach, AAMR abandoned a long
tradition still followed in the
DSM-
IV-TR
of dividing mental retardation into
four levels primarily based
on IQ scores: mild, moderate,
severe,
and
profound.
Levels
of Mental Retardation
1-
Mild mental retardation is the
designation for those with
IQ scores between 5055
and 70. People
with
mild mental retardation typically
have few, if any, physical
impairments, generally reach the
sixth-
grade
level in academic functioning, acquire
vocational skills, and typically
live in the community with
or
without special
supports.
2-
People
with moderate
mental retardation have
IQs between 3540 and
5055. They may
have
obvious
physical abnormalities such as the
features of Down syndrome.
Academic achievement
generally
reaches second-grade level, work
activities require close training
and supervision, and
special
supervision
in families or group homes is
needed for living in the
community.
3-
Severe mental retardation
is
defined by IQ scores between
2025 and 3540. At this
severity level,
motor
development typically is abnormal, communicative
speech is sharply limited,
and close
supervision
is needed for community
living.
4-
Profound mental retardation
is
characterized by an IQ below 2025.
Motor skills, communication,
and
self-care are severely
limited, and constant supervision is
required in the community or in
institutions.
·
A
diagnosis of mental retardation literally
might mean a difference between
life and death.
·
The
United States Supreme Court
recently ruled that the
death penalty is "cruel and
unusual
punishment"
for someone with mental
retardation, and therefore is
prohibited.
Frequency
of Mental Retardation
·
The
best estimate is that only 1
percent of the population has
mental retardation.
·
Mental
retardation in the United States is more
common among the poor and, as a
result, among
certain
ethnic groups.
210
Abnormal
Psychology PSY404
VU
Causes
of Mental Retardation
1-
Biological Abnormalities
About
one-half of all cases of
mental retardation are caused by
known biological
abnormalities.
i.
Down syndrome
·
The
most common known biological
cause of mental retardation is the
chromosomal disorder
Down
syndrome.
·
The
cause of Down syndrome is the
presence of an extra
chromosome.
·
The
incidence of Down syndrome is
related to maternal
age.
·
In
general, children and adults
with Down syndrome function
within the moderate to severe
range
of
mental retardation.
ii.
Fragile-X syndrome
·
Another
chromosomal abnormality, fragile-X
syndrome, is the most common known
genetic
cause
of
mental retardation.
·
Fragile-X
syndrome is indicated by a weakening or
break on one arm of the X
sex chromosomes,
and
it is transmitted genetically.
·
Not
all children with the
fragile-X abnormality have
mental retardation.
iii.
Phenylketonuria
·
Phenylketonuria
or PKU, is one of
these.
·
PKU
is caused by abnormally high levels of
the amino acid phenylalanine,
usually
due to the absence
of
or an extreme deficiency in phenylalanine
hydroxylase, an
enzyme that metabolizes
phenylalanine.
·
Retardation
typically progresses from the
severe to profound
range.
·
Fortunately,
PKU can be detected by blood
testing in the first several
days after birth.
2-
Infectious Diseases
·
Mental
retardation can also be caused by
various infectious diseases.
·
Damaging
infections may be contracted during
pregnancy, at birth, or in infancy to
early childhood.
i.
Rubella (German
measles) is a viral infection
that may produce few
symptoms in the mother but
can
cause
severe mental retardation and
even death in the developing
fetus.
ii.
The human immunodeficiency virus (HIV)
can be
transmitted from an infected mother to
a
developing
fetus.
·
The
effects on the child are
profound, including mental retardation,
visual and language
impairments,
and eventual death.
iii.
Syphilis is a
bacterial disease that is transmitted
through sexual
contact.
·
Infected
mothers can pass the disease
to the fetus.
·
If
untreated, syphilis produces a number of
physical and sensory
handicaps in the fetus,
including
mental
retardation.
·
One
infectious disease that occurs after
birth meningitis
can
cause mental retardation.
3-
Environmental Toxins
·
Exposure to a
variety of environmental toxins can
also cause mental
retardation.
·
Both
legal and illegal drugs pose
a risk to the developing fetus.
·
Toxins
also present a potential
hazard to intellectual development after
birth.
4-
Pregnancy and birth
complications
·
Pregnancy
and birth complications also
can cause mental
retardation.
·
One major
complication is Rh
incompatibility.
·
Another
pregnancy and birth complication
that can cause intellectual deficits is
premature birth.
·
Other
pregnancy and birth complications
that can cause mental
retardation include extreme
difficulties
in delivery, particularly anoxia,
or oxygen
deprivation; severe malnutrition; and
the seizure
disorder
epilepsy.
211
Abnormal
Psychology PSY404
VU
5-
Cultural-familial Retardation
·
As the term
suggests, cultural-familial retardation
tends to run in families and
is linked with
poverty.
·
A
controversial issue is whether this typically
mild form of mental retardation is
caused primarily by
genes
or by psychosocial disadvantage.
·
Grossly
abnormal environments can produce gross
abnormalities in intelligence.
·
Cultural-familial
retardation is found far more
frequently among the
poor.
·
Part
of this is explained by the fact that
lower intelligence causes lower
social status.
·
Impoverished
environments lack the stimulation
and
responsiveness
required to
promote children's
intellectual
and social skills throughout
their development.
Treatment:
Prevention and Normalization
Three
major categories of intervention are
essential in the treatment of mental
retardation.
·
First,
many cases of both organic
and cultural-familial mental retardation
can be prevented through
adequate
maternal and child health
care, as well as early
psycho-educational programs.
·
Second,
educational, psychological, and
biomedical treatments can help people
with mental
retardation
to raise their achievement
levels.
·
Third,
the lives of people with mental
retardation can be normalized through
mainstreaming in
public
schools and promoting care
in the community.
·
The
availability and use of good
maternal and child health
care is one major step
toward the
primary
prevention of many biological
causes of mental retardation.
·
Planning
for childbearing can also
help prevent mental
retardation.
·
Early
social and educational
interventions can lead to the
secondary prevention of
cultural-familial
retardation.
The
most important current secondary
prevention is
i.
Careful
assessment early in life is critical to
tertiary prevention.
ii.
Medical
screening is essential for
detecting conditions like
PKU.
iii.
Accurate
detection is important, because early
interventions can help.
iv.
Treatment of the
social and emotional needs of people
with mental retardation may include
teaching
basic
self-care skills, such as feeding,
toileting and dressing,
during the younger ages and
various "life-
survival"
skills at later ages.
v.
Medical
care for physical and
sensory handicaps is also critical in the
treatment of certain types of
mental
retardation. Medication is not especially
helpful in treating the intellectual or
socio-emotional
problems
of people with mental retardation.
vi.
Normalization
means that people with
mental retardation are entitled to
live as much as possible
like
other
members of society. The major
goals of normalization include
mainstreaming children
with
mental
retardation into public schools
and promoting a role in the community
for adults with
mental
retardation.
For
many children with mental
retardation, the least restrictive environment
means mainstreaming them
into
regular classrooms.
212
Table of Contents:
- ABNORMAL PSYCHOLOGY:PSYCHOSIS, Team approach in psychology
- WHAT IS ABNORMAL BEHAVIOR:Dysfunction, Distress, Danger
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Supernatural Model, Biological Model
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Free association, Dream analysis
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Humanistic Model, Classical Conditioning
- RESEARCH METHODS:To Read Research, To Evaluate Research, To increase marketability
- RESEARCH DESIGNS:Types of Variables, Confounding variables or extraneous
- EXPERIMENTAL REASEARCH DESIGNS:Control Groups, Placebo Control Groups
- GENETICS:Adoption Studies, Twin Studies, Sequential Design, Follow back studies
- RESEARCH ETHICS:Approval for the research project, Risk, Consent
- CAUSES OF ABNORMAL BEHAVIOR:Biological Dimensions
- THE STRUCTURE OF BRAIN:Peripheral Nervous System, Psychoanalytic Model
- CAUSES OF PSYCHOPATHOLOGY:Biomedical Model, Humanistic model
- CAUSES OF ABNORMAL BEHAVIOR ETIOLOGICAL FACTORS OF ABNORMALITY
- CLASSIFICATION AND ASSESSMENT:Reliability, Test retest, Split Half
- DIAGNOSING PSYCHOLOGICAL DISORDERS:The categorical approach, Prototypical approach
- EVALUATING SYSTEMS:Basic Issues in Assessment, Interviews
- ASSESSMENT of PERSONALITY:Advantages of MMPI-2, Intelligence Tests
- ASSESSMENT of PERSONALITY (2):Neuropsychological Tests, Biofeedback
- PSYCHOTHERAPY:Global Therapies, Individual therapy, Brief Historical Perspective
- PSYCHOTHERAPY:Problem based therapies, Gestalt therapy, Behavioral therapies
- PSYCHOTHERAPY:Ego Analysis, Psychodynamic Psychotherapy, Aversion Therapy
- PSYCHOTHERAPY:Humanistic Psychotherapy, Client-Centered Therapy, Gestalt therapy
- ANXIETY DISORDERS:THEORIES ABOUT ANXIETY DISORDERS
- ANXIETY DISORDERS:Social Phobias, Agoraphobia, Treating Phobias
- MOOD DISORDERS:Emotional Symptoms, Cognitive Symptoms, Bipolar Disorders
- MOOD DISORDERS:DIAGNOSIS, Further Descriptions and Subtypes, Social Factors
- SUICIDE:PRECIPITATING FACTORS IN SUICIDE, VIEWS ON SUICIDE
- STRESS:Stress as a Life Event, Coping, Optimism, Health Behavior
- STRESS:Psychophysiological Responses to Stress, Health Behavior
- ACUTE AND POSTTRAUMATIC STRESS DISORDERS
- DISSOCIATIVE AND SOMATOFORM DISORDERS:DISSOCIATIVE DISORDERS
- DISSOCIATIVE and SOMATOFORM DISORDERS:SOMATOFORM DISORDERS
- PERSONALITY DISORDERS:Causes of Personality Disorders, Motive
- PERSONALITY DISORDERS:Paranoid Personality, Schizoid Personality, The Diagnosis
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Poly Drug Use
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Integrated Systems
- SCHIZOPHRENIA:Prodromal Phase, Residual Phase, Negative symptoms
- SCHIZOPHRENIA:Related Psychotic Disorders, Causes of Schizophrenia
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:DELIRIUM, Causes of Delirium
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:Amnesia
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- PSYCHOLOGICAL PROBLEMS OF CHILDHOOD:Kinds of Internalizing Disorders
- LIFE CYCLE TRANSITIONS AND ADULT DEVELOPMENT:Aging