 |
SOCIAL PSYCHOLOGY APPLIED: SOCIAL PSYCHOLOGY IN CLINIC |
| << SOCIAL PSYCHOLOGY APPLIED: SOCIAL PSYCHOLOGY IN COURT |
| FINAL REVIEW:Social Psychology and related fields, History, Social cognition >> |
Social
Psychology (PSY403)
VU
Lesson
44
SOCIAL
PSYCHOLOGY APPLIED: SOCIAL
PSYCHOLOGY IN CLINIC
Aims:
�
To
understand the use of social psychology theories and
principles in clinical settings
Objectives:
�
To
discuss clinician's biases in
making clinical judgments
�
To
discuss the relationship of faulty
cognitions and mental and
physical illness
�
To
describe social-psychological approaches
to reverse the maladaptive patterns of
behavior
�
To
ascertain the relationship between
positive resources and
well-being
Chapter
Summary
This
chapter focuses on the social psychological
perspective on health and illness.
Health psychology is
based
on the biopsychosocial model, which
suggests that health and
illness are each multiply
determined by
biological,
psychological, and social factors. The
relationship between negative cognitions
and physical
and
mental health is discussed. Basic
attitudes that determine
health behaviors including
attitude toward
illness,
optimism vs. pessimism, and
explanatory styles are highlighted.
The importance of
positive
resources
and social support is reviewed in the
light of current research.
The ability of people to
recognize
their
physical symptoms is discussed as a
contributor to illness and
recovery. The interaction
between
patients
and practitioners is considered as a contributor to
low adherence to treatment programs,
and
interventions
that can improve adherence
are discussed. Discussing several methods
to reverse maladaptive
behaviors,
the chapter concludes by indicating that
the best treatment strategy is that patients
are equipped
with
the ability to have a control and mastery
over their negative
cognitions and maladapted
behavior.
Introduction:
Among
the many thriving areas of
applied social psychology is
one that relates social
psychology's
concepts
to depression, to other problems such as
loneliness, anxiety, and
physical illness, and now
to
happiness
and well-being. This bridge-building
research between social psychology
and clinical
psychology
seeks answers to four
important questions:
�
As
lay people or as professional
psychologists, how can we improve
our judgments and predictions
about
others?
�
How
can the ways in which we think
about self and others
feed such problems as
depression,
loneliness,
anxiety, and ill health?
�
How
might these maladaptive
thought patterns be
reversed?
�
What
part do close, supportive
relationships play in health and
happiness?
Making
clinical judgments
Social
psychologists are also interested to know
whether influences on our social
judgment also affect
clinicians'
judgments of clients. If so, what
biases should clinicians
(and their clients) be wary
of?
Is
Anjum suicidal? Should Ali be
admitted to a mental hospital? If
released Shaukat will be a
homicide
risk?
Facing such questions, clinical
psychologists struggle to make accurate
judgments, recommendations,
and
predictions.
Such
clinical judgments are also social
judgments and thus vulnerable to illusory
correlations,
overconfidence
bred by hindsight, and self-confirming
diagnoses. Professional clinicians are
"vulnerable to
insidious
errors and biases," concludes
James Maddux (1993).
Illusory
correlations
The
assumption here, as in so many clinical
judgments, is that test results
reveal something important.
Some
projective tests relate
people's responses (e.g.,
drawing big ears, bushy eyebrows,
pointed hands,
189

Social
Psychology (PSY403)
VU
figure
without feet, etc.) with
suspiciousness, hostility, anger,
conflicts, insecurity, etc.
Some tests are
indeed
predictive. Others, such as a
projective test, "Draw-a-Person",
has correlations far weaker
than their
users
suppose. Why, then, do
clinicians continue to express
confidence in uninformative or
ambiguous
tests?
Pioneering
experiments by Loren Chapman and Jean
Chapman (1969, 1971) helped
us see why. They
invited
both college students and
professional clinicians to study
some test performances and
diagnoses. If
the
students or clinicians expected a
particular association they generally
perceived it, regardless of
whether
the
data were supportive. For
example, clinicians who
believed that suspicious
people draw peculiar
eyes
on
the Draw-a-Person test perceived
such
Hindsight
bias
It
has often been criticized
that the clinicians are too
readily convinced of their
own after-the-fact
analyses.
If
someone we know commits suicide,
how do we react? One common
reaction is to think that
we, or those
close
to the person, should have been
able to predict and therefore to
prevent the suicide: In hindsight,
we
can
see the suicidal signs and
the pleas for help. One
experiment gave people a description of a
depressed
person
who later committed suicide.
Compared to those not informed of the
suicide, those told the
person
committed
suicide were more likely to say
they "would have expected" it
(Goggin & Range,
1985).
Moreover,
if they were told of the suicide,
their reactions to the victim's family
were more negative. After a
tragedy,
an I-should-have-known-it-all- along phenomenon
can leave family, friends,
and therapists feeling
guilty.
David
Rosenhan (1973) and his
seven associates provided a
striking example of potential
error in
after-the-
fact explanations. To test
mental health workers'
clinical insights, they each
made an appointment
with
a different mental hospital
admissions office and complained of
"hearing voices." Apart from
giving
false
names and vocations, they
reported their life
histories and emotional states
honestly and exhibited
no
further
symptoms. Most were diagnosed as schizophrenic and
remained hospitalized for two to
three
weeks.
Hospital clinicians then
searched for early incidents
in the pseudo-patients' life histories
and
hospital
behavior that confirmed and
"explained" the diagnosis.
Rosenhan
later told some staff
members (who had heard about
his controversial experiment but
doubted
such
mistakes could occur in their
hospital) that during the
next three months one or more
pseudo-patients
would
seek admission to their hospital.
After the three months, he asked the
staff to guess which of the
193
patients
admitted during that time
pseudo-patients were really. Of the 193
new patients, 41 were accused by
at
least one staff member of
being pseudo-patients. Actually, there were
none!
Overconfidence
A
third problem with clinical
judgment is that people may
also supply information that
fulfills clinicians'
expectations.
In a clever series of experiments at the
University of Minnesota, Mark
Snyder (1984), in
collaboration
with William Swann and others, gave
interviewers some hypotheses to
test concerning
individuals'
traits. Snyder and Swann
found that people often
test for a trait by looking
for information that
confirms
it. If they are trying to
find out if someone is an
extravert, they often
solicit instances of
extraversion
("What would you do if you
wanted to liven things up at a
party?"). Testing for
introversion,
they
are more likely to ask,
"What factors make it difficult
for you to really open up to
people?"
Clinical
versus statistical prediction
Given
these hindsight- and diagnosis-confirming
tendencies, it will come as no surprise
that most clinicians
and
interviewers express more confidence in
their intuitive assessments
than in statistical data
(such as
using
past grades and aptitude
scores to predict success in graduate or
professional college). Yet
when re-
searchers
pit statistical prediction against
intuitive prediction, the statistics
usually win.
Statistical
predictions
are indeed unreliable, but
human intuition-- even expert
intuition--is even more
unreliable.
Three
decades after demonstrating the
superiority of statistical over
intuitive prediction, Paul
Meehl (1986)
found
the evidence stronger than ever.
190
Social
Psychology (PSY403)
VU
Social
cognition in problem
behaviors
Negative
cognitions can be related to
host of problems as mentioned
below:
�
Social
cognition and depression
�
Social
cognition and loneliness
�
Social
cognition and anxiety
�
Social
cognition and illness
Social
cognition and
depression
As
we all know from experience,
depressed people are
negative thinkers. They view
life through dark-
colored
glasses. With seriously
depressed people--those who
are feeling worthless, lethargic,
uninterested
in
friends and family, and unable to
sleep or eat normally--the
negative thinking becomes
self-defeating.
Their
intensely pessimistic outlook leads them
to magnify bad experiences and minimize
good ones.
�
Depressive
realism is the tendency of mildly
depressed people to make
accurate rather than
self-
serving
judgments, attributions, and
predictions.
�
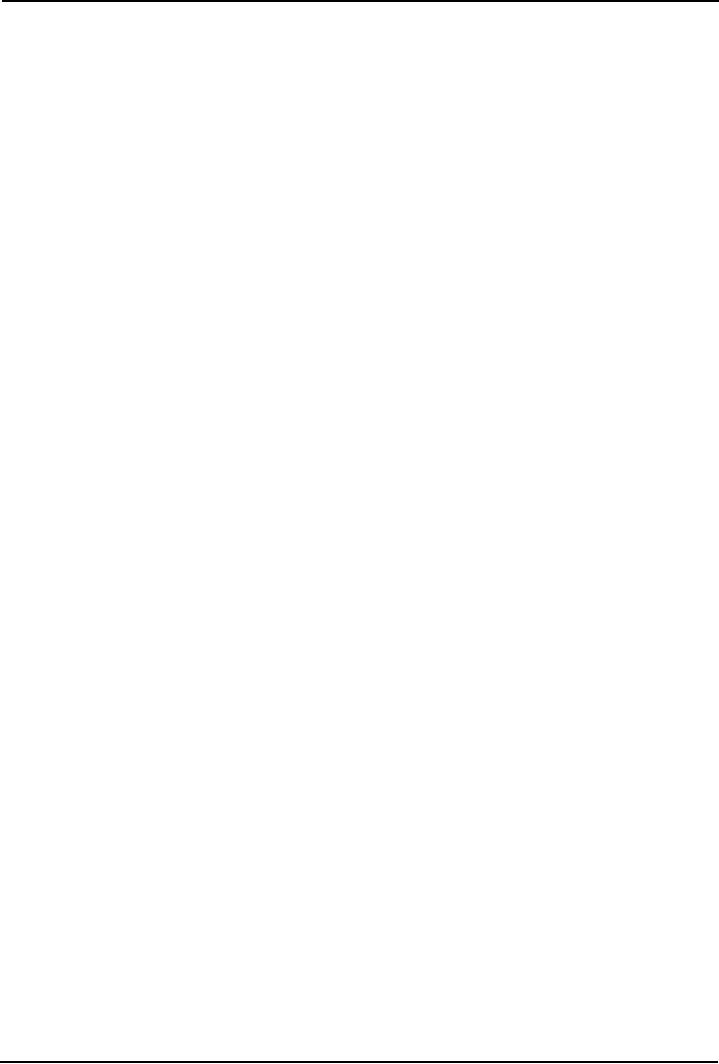
In
over 100 studies involving
15,000 subjects, depressed
people have been more likely
than
nondepressed
people to exhibit a negative
explanatory style (Sweeney et al.
1986)
Figure
1: Depressive explanatory
style
Is
negative thinking a cause or a
result of depression?
Depressed
moods cause negative
thinking
�
Currently
depressed people recall
their parents as having been
rejecting and punitive. But
formerly
depressed
people recall their parents
in the same positive terms as do
never-depressed people
(Lewinsohn
& Rosenbaum, 1987).
�
Edward
Hirt and his colleagues (1992)
demonstrated, in a study of Indiana
University basketball
fans,
that even a temporary bad mood
induced by defeat can darken
our thinking. After the
fans
were
either depressed by watching
their team lose or elated by a
victory, the researchers
asked
them
to predict the team's future performance,
and their own. After a
loss, people offered
bleaker
assessments
not only of the team's
future but also of their
own likely performance at
throwing
darts,
and solving anagrams. When
things aren't going our way,
it may seem as though they
never
will.
�
Being
depressed has cognitive and
behavioral effects: A depressed mood
also affects behavior.
The
person
who is withdrawn, glum, and
complaining does not elicit
joy and warmth in others.
Stephen
191
Social
Psychology (PSY403)
VU
Strack
and James Coyne (1983) found
that depressed people were
realistic in thinking that
others
didn't
appreciate their behavior. Their
pessimism and bad moods
trigger social rejection.
Depressed
behavior
can also trigger reciprocal
depression in others. College students
who have depressed
roommates
tend to become a little
depressed themselves. In couples, too,
depression is often
contagious
(Katz & others, 1999).
Negative
thinking causes depressed
mood
�
Negative
explanatory style contributes to
depressive reactions.
�
One
study monitored university
students every six weeks
for two and a half
years (Alloy & others,
1999).
Only one percent of those who
began college with
optimistic thinking styles had a first
de-
pressive
episode, but 17 percent of those with
pessimistic thinking styles did.
�
"A
recipe for severe depression is
preexisting pessimism encountering
failure," notes
Martin
Seligman
(1991, p. 78). Patients who
end therapy no longer feeling
depressed but retaining
a
negative
explanatory style tend to
relapse as bad events occur (Seligman,
1992). If those with
a
more
optimistic explanatory style
relapse, they often recover
quickly
�
Vicious
cycle of depression makes one more
vulnerable to depression (see
below in Figure 2)
Figure
2: Vicious cycle of
depression
Social
cognition and
loneliness
If
depression is the common cold of
psychological
Depressed
SELF
disorders,
then loneliness is the headache.
Loneliness,
FOCUSED
Mood
whether
chronic or temporary, is a painful
awareness that
AND
SELF
BLAMED
our
social relationships are less
numerous or meaningful
than
we desire. Jenny de Jong-Gierveld (1987)
observed in
her
study of Dutch adults that
unmarried and unattached
people
are more likely to feel
lonely.
But
loneliness need not coincide
with aloneness. One
can
feel
lonely in the middle of a party and one
can be utterly
alone
in a room. Chronically lonely
people seem caught in
Cognitive
Negative
a
vicious cycle of self-defeating social
cognitions and
and
Experiences
Behavioral
social
behaviors. When paired with
a stranger of the same
Consequence
sex
or with a first-year college roommate,
lonely students
s
are
more likely to perceive the other
person negatively
(Wittenberg
& Reis, 1986).
Adolescents
experience such feelings more commonly
than do adults. When beeped by an
electronic pager
at
various times during a week and
asked to record what they were
doing and how they felt,
adolescents
more
often than adults reported
feeling lonely when alone
(Larsen & others, 1982). Males and
females feel
lonely
under somewhat different
circumstances--males when isolated from
group interaction,
females
when
deprived of close one-to-one
relationships (Berg & McQuinn). As
many recently widowed
people
know,
the loss of a person with
whom one has been attached
can produce unavoidable feelings
of
loneliness
(Stroebe & others, 1996).
Social
cognition and
anxiety
Shyness
is a form of social anxiety characterized by
self-consciousness and worry
about what others
think.
Compared
to unshy people, shy, self-conscious
people (whose numbers include
many adolescents) see
incidental
events as somehow relevant to
themselves. Shown someone
they think is interviewing them
live
(actually
a videotaped interviewer), they
perceive the interviewer as less
accepting and interested in them
(Pozo
& others, 1991).
Shy,
anxious people also
overpersonalize situations, a tendency
that breeds anxious concern
and, in
extreme
cases, paranoia. They also
overestimate the extent to which
other people are watching
and
192

Social
Psychology (PSY403)
VU
evaluating
them. If their hair won't
comb right or they have a
facial blemish, they assume
everyone else
notices
and judges them accordingly. Moreover, shy
people often are conscious
of their self-consciousness.
They
wish they could stop
worrying about blushing,
about what others are
thinking, or about what to
say
next.
Social
cognition and
illness
�
Reactions
to illness
o
Noticing
symptoms
o
Explaining
symptoms: Am I sick?
o
Do I
need treatment?
o
Socially
constructed disorders (Small & others,
1991).
On
April 13, 1989, some
2,000 spectators assembled in an
Auditorium in
California,
USA, to enjoy music
performances by 600 secondary school
students.
Shortly
after the program began, the nervous
students began complaining to
one
another
of headaches, dizziness, stomachaches,
and nausea. Eventually
247
became
ill, forcing evacuation of the
auditorium. A fire department
treatment
operation
was set up on the lawn
outside. Later investigation
revealed nothing--no
diagnosable
illnesses and no environmental problems.
The symptoms subsided
quickly
and were not shared by the audience.
The instant epidemic, it
seemed, was
socially
constructed.
�
Emotions
and illness
�
Heart
disease has been linked
with a competitive, impatient,
and--the aspect that
matters--
anger-prone
personality (Matthews, 1988).
Under stress, reactive, anger-prone
"Type A"
people
secrete more of the stress hormones
believed to accelerate the buildup of
plaque on the
walls
of the heart's arteries.
�
Optimism
and health:
o
Link
between optimism & later good
health (Peterson et al.,
1988): In 1946
Harvard
University
students were assessed for
optimism, and in 1980 they were
reassessed. The
results
showed a link between early
optimism and later
health.
o
A
link between optimism and immunity to
common illnesses, like cold,
sore throat,
and
flu has been identified
(Scheier & Carver, 1991).
�
Stress
and illness
o
People
who undergo highly stressful
experiences become more vulnerable to
disease
The
death of a spouse, the stress of a space
flight landing, even the strain of an
exam week
o
have
all been associated with
depressed immune defenses (Jemmott &
Locke, 1984)
�
Explanatory
style and illness
o
As
defined earlier, negative
and pessimistic explanatory styles are
related with poor
outcomes
in mental and physical
health.
Social-psychological
approaches to treatment
Inducing
internal change through external
behavior
Consistent
with this attitudes-follow-behavior
principle, several psychotherapy techniques prescribe
action.
Behavior
therapists try to shape behavior and
assume that inner
dispositions will tag along
after the
behavior
changes. Assertiveness training employs
the foot-in-the-door procedure. The
individual first
role-
plays
assertiveness in a supportive context,
then gradually becomes
assertive in everyday life.
Rational-
emotive
therapy assumes that we
generate our own emotions;
clients receive "homework"
assignments to
talk
and act in new ways that
will generate new
emotions.
193

Social
Psychology (PSY403)
VU
Breaking
vicious cycles
If
depression, loneliness, and social
anxiety maintain themselves
through a vicious cycle of
negative
experiences,
negative thinking, and
self-defeating behavior, it should be
possible to break the cycle at
any
of
several points--by changing the
environment, by training the person to
behave more constructively, by
reversing
negative thinking. Several different
therapy methods help free
people from depression's
vicious
cycle.
Engaging
in Social skills training
Depression,
loneliness, and shyness are
not just problems in someone's
mind. To be around a
depressed
person
for any length of time
can be irritating and
depressing. As lonely and shy
people suspect, they
may
indeed
come across poorly in social
situations. In these cases,
social skills training may
help. By observing
and
then practicing new
behaviors in safe situations, the
person may develop the
confidence to behave
more
effectively in other
situations.
Explanatory
style therapy
The
vicious cycles that maintain
depression, loneliness, and shyness
can be broken by social skills
training,
by
positive experiences that
alter self-perceptions, and by changing
negative thought patterns. Some
people
have
social skills, but their
experiences with hypercritical
friends and family have convinced them
they do
not.
For such people it may be
enough to help them reverse
their negative beliefs about
themselves and
their
futures. Among the cognitive therapies
with this aim is an
explanatory style therapy proposed
by
social
psychologists.
One
such program taught
depressed college students to
change their typical
attributions. Mary
Anne
Layden
(1982) first explained the
advantages of making attributions more
like those of the
typical
nondepressed
person (by accepting credit
for successes and seeing how
circumstances can make things
go
wrong).
After assigning a variety of tasks,
she helped the students see
how they typically
interpreted
success
and failure. Then came the
treatment phase: Layden instructed
each person to keep a diary of
daily
successes
and failures, noting how
they contributed to their
own successes and noting
external reasons for
their
failures. When retested
after a month of this
attributional retraining and compared
with an untreated
control
group, their self-esteem had risen and
their attributional style had
become more positive. And
the
more
their explanatory style
improved, the more their depression
lifted. By changing their
attributions, they
had
changed their emotions.
Maintaining
change through internal
attributions for
success
�
Once
improvement is achieved, it endures
best if people attribute it to factors
under their own
control
rather than to a treatment
program.
�
More
recent focus less on the therapist
than on how the interaction affects the
client's thinking
(Neimeyer
et al., 1991)
�
The
thoughtful central route to
persuasion provides the most
enduring attitude and
behavior
change.
Social
support and well-being
There
is one other major topic in the
social psychology of mental and
physical well-being. Supportive
close
relationships--feeling
liked, affirmed, and encouraged by
intimate friends and
family--predict both
health
and
happiness. However, relationships
are associated with both
stress and happiness.
�
Our
relationships are fraught
with stress.
�
"Hell
is others," wrote Jean-Paul
Sartre
�
Still,
on balance, close relationships
contribute less to illness
than to health and
happiness.
194

Social
Psychology (PSY403)
VU
Close
relationships and health
�
Those
who have close relationships
with friends, kin, or other
members of close-knit religious
or
community
organizations are less
likely to die prematurely.
And losing such ties heightens the
risk
of
disease.
�
A
Finnish study of 96,000
widowed people found their
risk of death doubled in the week
following
their
partner's death (Kaprio & others,
1987).
�
A
National Academy of Sciences
study reveals that those who
are recently widowed become
more
vulnerable
to disease and death (Dohrenwend &
others, 1982).
�
Among
the elderly, those having
long-term close relationships
with less than three people
were
much
more likely to die in the next three
years (Cerhan & Wallace,
1997).
�
In
more than 80 studies, social support has
been linked with better
functioning cardiovascular and
immune
systems (Uchino & others,
1996).
Close
relationships and happiness
�
Friendships and
happiness
o
Being
attached to friends with
whom we can share intimate
thoughts has two effects,
"It
redoubleth
joys, and cutteth griefs in
half" (Francis Bacon).
�
Marital
attachment and happiness
o
Compared to
those single or widowed, and
especially compared to those
divorced or
separated,
married people report being
happier and more satisfied with
life (Inglehart,
1990)
�
The
tighter social bonds of collectivist
cultures offer protection from
loneliness, alienation,
divorce,
and
stress-related diseases.
Readings:
�
David
G. Myers, D. G. (2002). Social
Psychology (7th ed.). New
York: McGraw-Hill.
Taylor,
S.E. (2006). Social
Psychology (12th ed.). New York: Prentice
Hall.
�
195
Table of Contents:
- INTRODUCTION TO SOCIAL PSYCHOLOGY:Readings, Main Elements of Definitions
- INTRODUCTION TO SOCIAL PSYCHOLOGY:Social Psychology and Sociology
- CONDUCTING RESEARCH IN SOCIAL PSYCHOLOGY:Scientific Method
- CONDUCTING RESEARCH IN SOCIAL PSYCHOLOGY:Evaluate Ethics
- CONDUCTING RESEARCH IN SOCIAL PSYCHOLOGY RESEARCH PROCESS, DESIGNS AND METHODS (CONTINUED)
- CONDUCTING RESEARCH IN SOCIAL PSYCHOLOGY OBSERVATIONAL METHOD
- CONDUCTING RESEARCH IN SOCIAL PSYCHOLOGY CORRELATIONAL METHOD:
- CONDUCTING RESEARCH IN SOCIAL PSYCHOLOGY EXPERIMENTAL METHOD
- THE SELF:Meta Analysis, THE INTERNET, BRAIN-IMAGING TECHNIQUES
- THE SELF (CONTINUED):Development of Self awareness, SELF REGULATION
- THE SELF (CONTINUE…….):Journal Activity, POSSIBLE HISTORICAL EFFECTS
- THE SELF (CONTINUE……….):SELF-SCHEMAS, SELF-COMPLEXITY
- PERSON PERCEPTION:Impression Formation, Facial Expressions
- PERSON PERCEPTION (CONTINUE…..):GENDER SOCIALIZATION, Integrating Impressions
- PERSON PERCEPTION: WHEN PERSON PERCEPTION IS MOST CHALLENGING
- ATTRIBUTION:The locus of causality, Stability & Controllability
- ATTRIBUTION ERRORS:Biases in Attribution, Cultural differences
- SOCIAL COGNITION:We are categorizing creatures, Developing Schemas
- SOCIAL COGNITION (CONTINUE…….):Counterfactual Thinking, Confirmation bias
- ATTITUDES:Affective component, Behavioral component, Cognitive component
- ATTITUDE FORMATION:Classical conditioning, Subliminal conditioning
- ATTITUDE AND BEHAVIOR:Theory of planned behavior, Attitude strength
- ATTITUDE CHANGE:Factors affecting dissonance, Likeability
- ATTITUDE CHANGE (CONTINUE……….):Attitudinal Inoculation, Audience Variables
- PREJUDICE AND DISCRIMINATION:Activity on Cognitive Dissonance, Categorization
- PREJUDICE AND DISCRIMINATION (CONTINUE……….):Religion, Stereotype threat
- REDUCING PREJUDICE AND DISCRIMINATION:The contact hypothesis
- INTERPERSONAL ATTRACTION:Reasons for affiliation, Theory of Social exchange
- INTERPERSONAL ATTRACTION (CONTINUE……..):Physical attractiveness
- INTIMATE RELATIONSHIPS:Applied Social Psychology Lab
- SOCIAL INFLUENCE:Attachment styles & Friendship, SOCIAL INTERACTIONS
- SOCIAL INFLUENCE (CONTINE………):Normative influence, Informational influence
- SOCIAL INFLUENCE (CONTINUE……):Crimes of Obedience, Predictions
- AGGRESSION:Identifying Aggression, Instrumental aggression
- AGGRESSION (CONTINUE……):The Cognitive-Neo-associationist Model
- REDUCING AGGRESSION:Punishment, Incompatible response strategy
- PROSOCIAL BEHAVIOR:Types of Helping, Reciprocal helping, Norm of responsibility
- PROSOCIAL BEHAVIOR (CONTINUE………):Bystander Intervention, Diffusion of responsibility
- GROUP BEHAVIOR:Applied Social Psychology Lab, Basic Features of Groups
- GROUP BEHAVIOR (CONTINUE…………):Social Loafing, Deindividuation
- up Decision GROUP BEHAVIOR (CONTINUE……….):GroProcess, Group Polarization
- INTERPERSONAL POWER: LEADERSHIP, The Situational Perspective, Information power
- SOCIAL PSYCHOLOGY APPLIED: SOCIAL PSYCHOLOGY IN COURT
- SOCIAL PSYCHOLOGY APPLIED: SOCIAL PSYCHOLOGY IN CLINIC
- FINAL REVIEW:Social Psychology and related fields, History, Social cognition