 |
Higher Order Brain Functions:Brain correlates, Handedness, Frontal lobe |
| << Higher Order Brain Functions:Principle of Mass Action, Long-term memory |

Neurological
Basis of Behavior (PSY -
610)
VU
Lesson45
Higher
Order Brain Functions
Objectives:
The
students would be familiarized
with the Brain Hemispheric
differences, Laterality, specialized
role
of
higher order brain
functioning. Brain Damage and
behaviors. Neuropsychological testing
would also
be
discussed
Brain
correlates:
·
Brain
correlates of Learning and Memory,
Amnesia, Verbal, Non verbal
memory,
(Neuropsychological
tools)
·
Split
Brain studies, Brain
Hemispheric differences, laterality
One brain/Two Brains?
Brain
Damage
and Plasticity
·
Neuropsychological
Tests
·
Cerebral
hemispheric specialization
Have
you ever wondered why we
have two lobes instead of one? Do they
work as one brain or two?
Are
they
independent or do they communicate with
each other. Is there any hemispheric
specializations
(doesn't
seem possible if you know
that all neuroanatomical
areas are bilaterally
located, right?). But
did
you know that brain
areas are not exactly
alike, and that each
command center deals with
the
opposite
hemisphere. All fibers cross over except
for the visual pathways, which
are partially
crossed.
This
makes for a very complex
research area, which was
only focused in the last few
decades.
Fact:
The
two lobes are connected by
commissures.
Fact:
There
are specializations of functions.
Fact:
There
is cooperation as well as competition
between the two hemispheres.
The
earliest study reported on the
"specialization" of brain hemispheric
specialization was reported by
a
French
Neurologist Marc Dax. Dax
presented his report on the
findings of brain autopsies in
a
conference
in 1836. The interesting
findings were that patients with
strokes, who had speech
problems
brain
damage, all had damage to the
left (none in the right hemisphere).
Not until 25 years later
did
some
one bring this to the attention of the
world obvious functional
specialization is speech
and
language
abilities. In the mid-1800s, Paul Broca
(a French neurosurgeon) reported two
cases of aphasia
where
the left hemisphere damage and
speech production was
identified. This is now
known as Brocas
area
(for
speech articulation. Shortly afterwards,
a German neurologist, Carl Wernicke,
identified
another
part of the left hemisphere
primarily concerned with language
comprehension (Wernicke's
area)
Two
studies in 1959 and 1961 produced
evidence that unilateral lesions produced
deficits which were
evidence
for brain hemispheric
specialization.
Roger
Penfield and his colleague
Ebert (1959) reports on neurological
patients and Russel and Sapir
(1961)
on military personnel. Their results
indicated that language was
dominant in left hemisphere
for
both
the left and the right hemispheric
dominant persons. (Remember: If you
are right hemisphere
dominant,
you are left handed, if you
are left hemisphere dominant
then you are right
handed)
Brain
Hemispheres: Two Brains or
One?
The
interest in further research in this
area was stimulated
accidentally. The major
names in this area
are
Penfield,
Sperry, Gazzaniga, Milner, and
many others who were pioneers in
this area
177

Neurological
Basis of Behavior (PSY -
610)
VU
These
studies used Commissurotomy, or
Split Brain Procedure. This
procedure uses a knife cut to
sever
the
commissures (including the Corpus
Callosum) so that the two
hemispheres cannot communicate
with
each other. Interesting
things happened. Outwardly these
individuals seem normal, but
sensitive
neuropsychological
tests revealed that there were
deficits. These tests were
visual tactual verbal
etc.
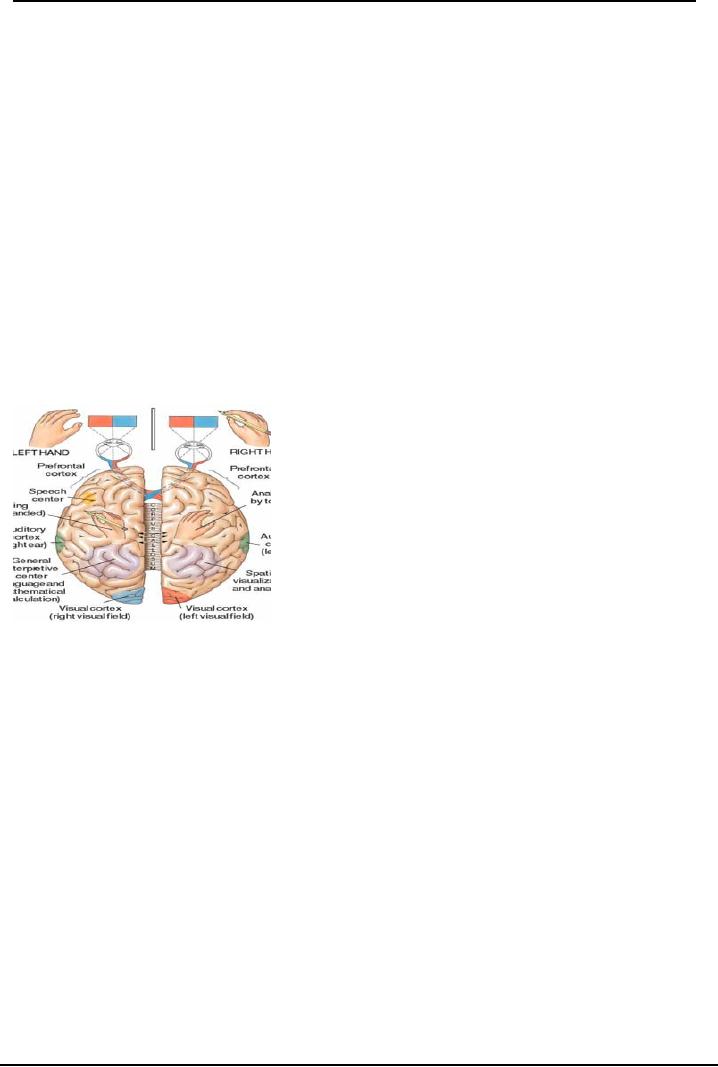
These
tests were devised so that information
could go to only one hemisphere.
When words were
presented
to the right visual field to
reach the left hemisphere, the person
could read it out loud
(and also
write
it). But then when it
was shown to the right hemisphere the
person reported he saw
nothing. The
right
hemisphere did not
comprehend? Or perceive? It was thought
that the left hemisphere did
all the
work,
and the right only was in a
supportive role. It could
not talk about what it saw,
but when the
methodology
was changed and the person
was asked to pick out words
from a group of alphabets or
objects
form a group of objects, he picked the
right ones!
When
HEART
was
flashed on the screen in such a
way that HE
was
in the right visual field so
that it
input
only the left hemisphere and
ART
input
to the right. When asked
what he saw, he stated HE,
but
when
asked to pick out words form
a bloc of words given, he picked
ART!
In
other studies, when a split
brain patient was walking
through the room he acted as a
blind man not
able
to see while he walked, but
he could identify objects in the areas
when asked verbalize.
Thus
do we have two brains or one, this is the
question researchers asked,
and what is the role of
each
Brain
Lateralization exists and the two halves
of the human brain are not
exactly alike. Each
hemisphere
has
functional specializations: some
function whose neural
mechanisms are localized
primarily in one
half
of the brain.
Handedness:
Handedness
as
(a)
The
hand that performs faster or more precisely on
manual tests, while others
define it as
(b)
The
hand that one prefers to use, regardless
of performance.
Majority
of us are right handers
(left hemisphere dominant),
but there are reasonable number of
people
who
are left handed, and a small number is
ambidextrous. Famous left
handers are Leonardo Da
Vinci,
Michelangelo,
Napoleon, Alexander the great, and Baden
Powel (ambidextrous: means
can use both
with
equal proficiency)
We
also have dominance for foot
(which foot used for
kicking a ball or stepping on a
stair first), eye (if
you
are to use a telescope which
eye would you use), ear
(which ear do you use
for listening to the
telephone).
Dominance can be assessing by
tests such as the Harris
Tests of Lateral Dominance.
Asymmetry
in faces is also reported,
and Sackheim, Gur and Saucy
(1978) took photographs of
expressed
emotions and cut them and made composites,
left-left (left half face) composite,
right-right
composite
(right half face composite), and had
subject compared it with normal pictures
for intensity of
emotions.
They found that subjects
reported the left-left faces more intense
as compared to the right
right
(why? Because the right
hemisphere cannot speak, so images have
to be more intense for the visual
input,
whereas the left hemisphere
can express itself through
words.
How
do we explain asymmetry?
There
are two schools of thought
a) one which believes that
the: brain is equipotential
for specialization
and
at around 2 years of age the
division of labor and specializations of the
two hemispheres is
completed.
The two hemispheres compete
for control e.g. when both
try to speak at the same
time
stuttering
occurs, Orton (1939).
178

Neurological
Basis of Behavior (PSY -
610)
VU
The
other view point is that it
is inborn and innate. This is even
before any cultural or
learning
influences
can take place. For example,
the planum temporale in the left
hemisphere is larger in the
fetus.
Therefore language is programmed to be in the left
hemisphere
Tests
for Language and Other
Functions.
a)
The WADA test: In this
test Sodium Amytal, a
barbiturate is injected through the
carotid
arteries
(main arteries which carry
blood to the brain). This
injection is made unilaterally
(to one
hemisphere
only) and the patient is required to
speak a list of words. When
the language
hemisphere
is anaesthetized, the patient's speech
becomes slurred, till it is
blocked completely.
Milner
branch and Rasmussen (1966) studied
212 patients like this to
identify hemispheric
dominance
for speech.
b)
Zeidel
lens (a specialized
tachistoscope) was used to
project images only to one
hemisphere to
test
verbal, visual, language and other
asymmetries.
c)
Dichotic
listening tests: this is a
test which sends out
two different types of auditory signals
to
the
left and the right ear.
For example, it can send
alphabets to the left ear and
simultaneously
send
out numbers to the right ear.
The subject is asked to repeat
what they hear. The
dominant
ear
would hear, and therefore the list
given by the subject would be of what the
dominant ear
heard.
At
present research is ongoing and it
has been recognized that
each hemisphere is specialized to
work
alone
and to work together.
Unilateral
neglect, unilateral sensory
neglect
This
is very special disorder affecting
response to one side of the
body, somato-sensory, or visual
field.
It
is characterized by the patient not
attending to one side only.
This occurs as a consequence of
damage
to
either hemisphere in the spatial
recognition the parieto-occipital
area.
This is a lateralized deficit
i.e.
the
patients don't respond to the side/
visual field opposite to
damaged hemisphere. How can
we assess
this
simply by asking the patient to
draw a clock face with
numbers and showing a specific
time let's
say
10 to 11 o'clock. And the patient
draws only one half of the
clock. In extreme cases the patients
eat
from
one side of plate, or shave one
side of face, put lipstick
on only half the face, interestingly if
we
move
them around they are able to
describe the whole as their
body moves.
More
interesting and intriguing is the finding
that we may have our frontal
cortex controlling the rest
of
the
body and brain, as the Chief
executive.
Frontal
lobe
Orbit
frontal: there is an
interesting paper entitled No Longer
Gage. This is
about a person named
Phineas
Gage who was a railway
laborer. During construction, he had a
major head injury where the
rod
he
was holding went right
through his head. He
survived but he changed
personality, he was no
longer
the
same person. His family
and friends said- he was no
longer Gage. It was found
that his injury to
the
Orbito
frontal areas changed him.
There is now much research
which indicates that
judgment,
personality,
fore sight, "conscience"
reduced impulsivity are all
located in this area. As a
child grows,
inhibitions
of the society and culture
learning are all programmed in
this area. Similarly control
of all
emotions
also resides here.
·
Neuropsychological
tests:
a)
Luria,
the father of Neuropsychology developed a
series of tests to assess
all abilities, but
holistically
and
by varying the tasks. For
example to test handed ness, he
would give the same task
but use different
179
Neurological
Basis of Behavior (PSY -
610)
VU
modalities
(visual, somato-sensory: touch, language
command etc) different tests).
These have been
incorporated
in the Luria Nebraska Nueropsychological
test Battery
b)
Halstead
Reitan Battery also tests
such as the grooved pegboard, the tapping
tests etc.
·
Harris
tests of laterality
Research
ongoing but both hemispheres
work and compete, they are
working together, sharing
information
through corpus callosum this
gives ones behavior a
holistic, and a gestalt. Each
hemisphere
needs the other, to provide back up
information.
What
if one hemisphere only? There have
been cases where through surgery or
brain injury or even
birth
or developmental trauma, one hemisphere
has been lost
If
there is only one hemisphere, the remaining
hemisphere can take over
functions- without
any
visible
or other deficits. The
earlier the traumas the more easily
can the functioning take place.
In
later
life, it becomes difficult
for the hemisphere to
relearn.
Neuropsychological
Tests
Neuropsychological
assessment of cognition and other
functions is carried out by
trained
neuropsychologists
(brain-behavior relationship
specialists).
A
formal interview is carried
out initially followed by
review of all medical and
other history taking
records
(whether they have been treated,
birth traumas school records,)
interviews of parents, or
relatives
and neuropsychological testing using
formalized procedure and tests
Neuropsychological
testing aims to assess a
patient's higher order
functioning of attention,
memory,
speed
of information processing, language,
visual-spatial ability, sensory
processing, motor
ability,
executive
and intellectual functioning. This is
based on the referral questions and also
the previous
history
of the patient. This also helps in
developing a rehabilitation
strategy.
The
referrals for neuropsychological
assessments are
a)
Stroke
patients
b)
Head
injury patients
c)
Children
with slow development or
difficulties in speech, attention or
learning
d)
Chronic
alcohol or substance
abusers
180

Neurological
Basis of Behavior (PSY -
610)
VU
Some
neuropsychological tests
There
are several protocols available, the
two well known batteries are
a) The Halstead
Reitan
Neuropsychological
Battery is older and
which takes about 8 hours
for a patient to complete.
The
second
battery is the Luria-
Nebraska Neuropsychological Test Battery
which
is developed by
American
Neuropsychologists based on Luria's
techniques. This is has a series of
subtests but takes
less
time
and has more flexibility
(qualitative information). These
tests assess motor, sensory,
visual
language,
kinesthetic, attention, memory,
receptive and expressive speech
(speech sounds rhythm)
tests.
Test
also assess if the patient is
following instructions through
different modal tests
Two
of the simplest tests which I have used
which provide rich
information are the Trails
making A
and
B: these
are part of the Halstead Reitan
Battery. They appear simple
where the patient has to
join
lines
of various numbers in Part A and
numbers and words in alternating sequence
in Part B. Spatial
organization,
grapho-motor speed, recognition of
numbers, visual pursuit,
vigilance and number
sequences
is measured by this. Part
A evaluates
visual motor coordination
and visual scanning as
well
as
short term memory. Part
B measures
higher order functioning as it requires
alternating between
numbers
and letters, ability to learn an
organizing principle and apply it
systematically, also
verbal
problem
solving, and planning action
beforehand.
Thus,
the Neuropsychological tests are
effective tools for a
trained person. These tests
are used for
diagnosis,
to identify deficits due to illness or
injury, to assess learning problems,
reasoning and
problem
solving abilities, ability to understand
and express language, memory and
attention especially
post
trauma, visual-spatial memory and
organization, visual-motor coordination,
and higher order
planning
and organizing abilities.
Course
Recap
We
have completed the course today,
and if we look where our
lessons began.
a)
We
learnt about the development of
behavioral Neurosciences as a discipline,
the major
contributors
to this discipline, and how it is
made up of specializations from various
field of the
hard
sciences Chemistry, biochemistry,
physics, biology and of course
this is incorporated to
help
us understand behavior- both at the lower
level (of animals) and of
humans
b)
We
learnt of the various stages of
evolutionary development, of
commonalities and differences
between
man and other animals. We
also learnt of how the brain
developed form a single
cell
layer
to the complex form we have. The
developmental journey with
nature- nurture
interaction,
where
things can go as programmed if only the
right environmental stimulation is
given
c)
You
also learnt about the
various neuroanatomical sites and
their contribution to
behavior,
NeuroChemicals
and their effect (in
some cases very serious
psychopathologies and
physiological
deficits can take place with
a single molecule
d)
We
have learnt how motivational
states are neuro-anatomically,
neuro-chemically driven.
Hunger,
thirst, sleep, without which
we may not be able to
survive let alone
function
e)
The
journey into higher order
functioning, language (its deficits)
learning and memory
(amnesias),
disorders such as apraxias, agnosias,
aphasias, were also discussed
giving you and
insight
into the neuropsychological
area
f)
It
ahs always been interesting
to teach the brain-behavior
relationships, I do hope this
course
would
help you understand your
behavior as well as behavior of
others better.
181

Neurological
Basis of Behavior (PSY -
610)
VU
There
are excellent sites on the web for you to visit and learn more. Some of them are
given in the
handouts,
but others are as follows:
Central
Nervous System Overview
Learn
about an astonishingly complex system of creases, projections, fibers, branching
cells, colors, and
connections
known as the human nervous system.
http://www.brainconnection.com/topics/?main=anat/cns
Primate
Handedness and Brain Lateralization
By
M.K. Holder, Ph.D.
http://www.indiana.edu/~primate/
References:
1.
Carlson N.R. (2005) Foundations of
Physiological Psychology Allyn and Bacon,
Boston
2.
Pinel, John P.J. (2003)
Biopsychology (5th edition) Allyn and Bacon
Singapore
3.
Bloom F, Nelson and Lazerson (2001),
Behavioral Neuroscience: Brain, Mind
and Behaviors (3rd
edition)
Worth Publishers New
York
4.
Bridgeman, B (1988) The
Biology of Behaviour and Mind. John
Wiley and Sons New
York
5.
Brown,T.S. and Wallace.(1980) P.M
Physiological Psychology. Academic
Press New York.
6.
Bradshaw J.L. and Mattingley,
J.B. (1995) Clinical
Neuropsychology: Behavioral and
Brain
Sciences.
ACADEMIC PRESS
182
Table of Contents:
- INTRODUCTION:Descriptive, Experimental and/ or Natural Studies
- BRIEF HISTORICAL REVIEW:Roots of Behavioural Neurosciences
- SUB-SPECIALIZATIONS WITHIN THE BEHAVIORAL NEUROSCIENCES
- RESEARCH IN BEHAVIOURAL NEUROSCIENCES:Animal Subjects, Experimental Method
- EVOLUTIONARY AND GENETIC BASIS OF BEHAVIOUR:Species specific
- EVOLUTIONARY AND GENETIC BASIS OF BEHAVIOUR:Decent With Modification
- EVOLUTIONARY AND GENETIC BASIS OF BEHAVIOUR:Stereoscopic vision
- GENES AND EXPERIENCE:Fixed Pattern, Proteins, Genotype, Phenotypic
- GENES AND EXPERIENCE:Mendelian Genetics, DNA, Sex Influenced Traits
- GENES AND EXPERIENCE:Genetic Basis of behavior, In breeding
- GENES AND EXPERIENCE:Hybrid vigor, Chromosomal Abnormalities
- GENES AND EXPERIENCE:Behavioral Characteristics, Alcoholism
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION:Activating brain
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION:Macro electrodes
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION:Water Mazes.
- DEVELOPMENT OF THE NERVOUS SYSTEM:Operation Head Start
- DEVELOPMENT OF THE NERVOUS SYSTEM:Teratology studies, Aristotle
- DEVELOPMENT OF THE NERVOUS SYSTEM:Stages of development, Neurulation
- DEVELOPMENT OF THE NERVOUS SYSTEM:Cell competition, Synaptic Rearrangement
- DEVELOPMENT OF THE NERVOUS SYSTEM:The issues still remain
- DEVELOPMENT OF THE NERVOUS SYSTEM:Post natal
- DEVELOPMENT OF THE NERVOUS SYSTEM:Oxygen level
- Basic Neuroanatomy:Brain and spinal cord, Glial cells, Oligodendrocytes
- Basic Neuroanatomy:Neuron Structure, Cell Soma, Cytoplasm, Nucleolus
- Basic Neuroanatomy:Control of molecules, Electrical charges, Proximal-distal
- Basic Neuroanatomy:Telencephalon, Mesencephalon. Myelencephalon
- Basic Neuroanatomy:Tegmentum, Substantia Nigra, MID BRAIN areas
- Basic Neuroanatomy:Diencephalon, Hypothalmus, Telencephalon, Frontal Lobe
- Basic Neurochemistry:Neurochemicals, Neuromodulator, Synaptic cleft
- Basic Neurochemistry:Changes in ionic gates, The direct method, Methods of Locating NT
- Basic Neurochemistry:Major Neurotransmitters, Mesolimbic, Metabolic degradation
- Basic Neurochemistry:Norepinephrine/ Noradrenaline, NA synthesis, Noadrenergic Pathways
- Basic Neurochemistry:NA and Feeding, NE and self stimulation: ICS
- Basic Neurochemistry:5HT and Behaviors, Serotonin and sleep, Other behaviours
- Basic Neurochemistry:ACH and Behaviors, Arousal, Drinking, Sham rage and attack
- Brain and Motivational States:Homeostasis, Temperature Regulation, Ectotherms
- Brain and Motivational States:Biological Rhythms, Circadian rhythms, Hunger/Feeding
- Brain and Motivational States:Gastric factors, Lipostatic theory, Neural Control of feeding
- Brain and Motivational States:Resting metabolic state, Individual differences
- Brain and Motivational States:Sleep and Dreams, Characteristics of sleep
- Higher Order Brain functions:Brain correlates, Language, Speech Comprehension
- Higher Order Brain functions:Aphasia and Dyslexia, Aphasias related to speech
- Higher Order Brain Functions:Principle of Mass Action, Long-term memory
- Higher Order Brain Functions:Brain correlates, Handedness, Frontal lobe